Mirena IUD and the Postpartum Breastmilk Supply Paradox
As a mother, you are finally finding a rhythm with exclusive breastfeeding, shielding that fragile supply with everything you have. Then you hit 6 weeks and are asked if you want an IUD. As a scientist, I understand the necessity of a highly effective, low-maintenance contraceptive to protect our reproductive health and allow our bodies to heal but the digital whispers in breastfeeding communities tell a much more alarming story of supply "tanking" overnight. This, my friends, is the "Postpartum Paradox".
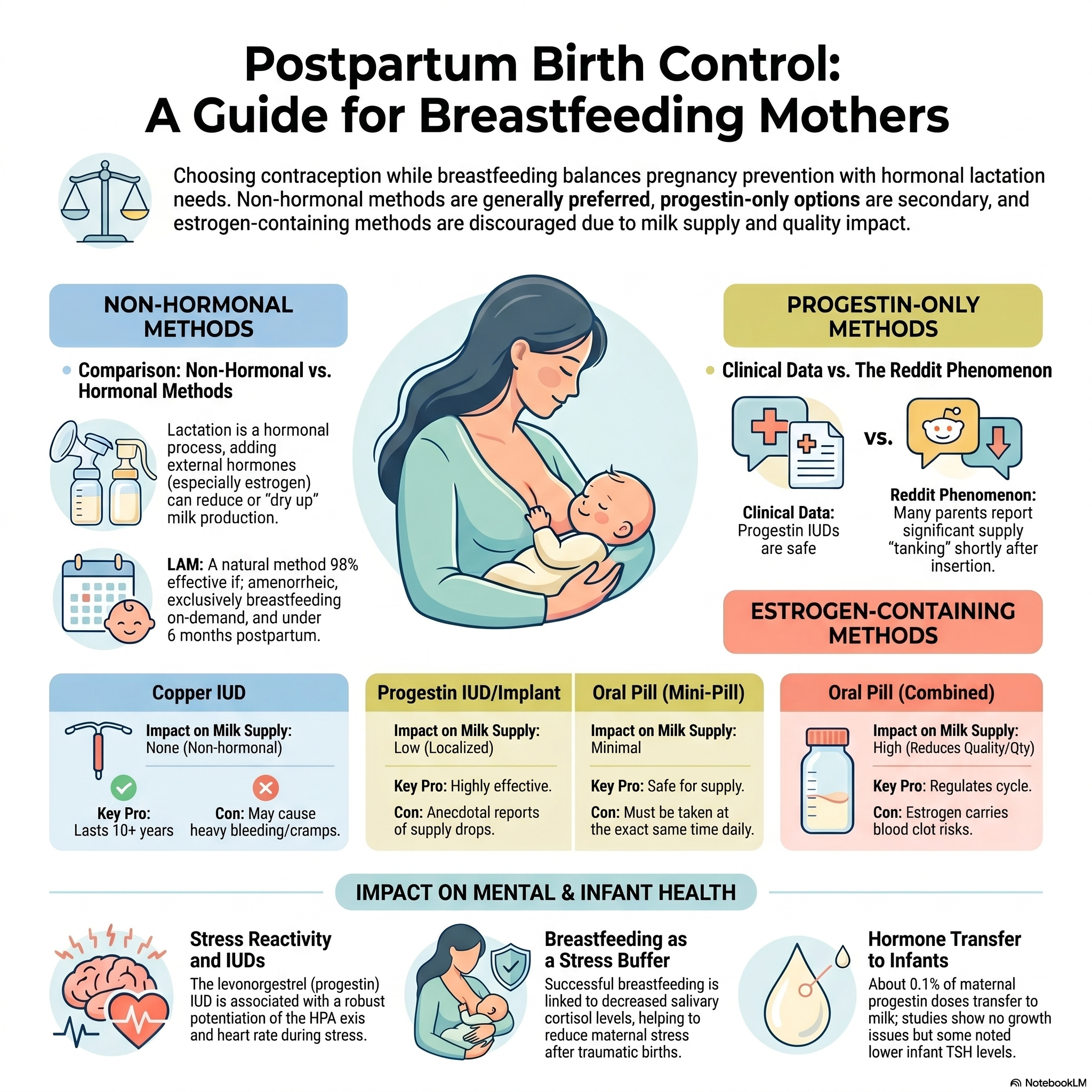
Choosing between reliable contraception and your breastfeeding goals should not be a gamble based on luck. To make an empowered decision, let’s dive in and bridge the gap between clinical data and the individual physiological reality.
Why Does The Supply Dip?
When a mother reports a sudden loss of milk following an IUD insertion, we must look at two distinct biological pathways: the acute physical response and the chronic hormonal influence.
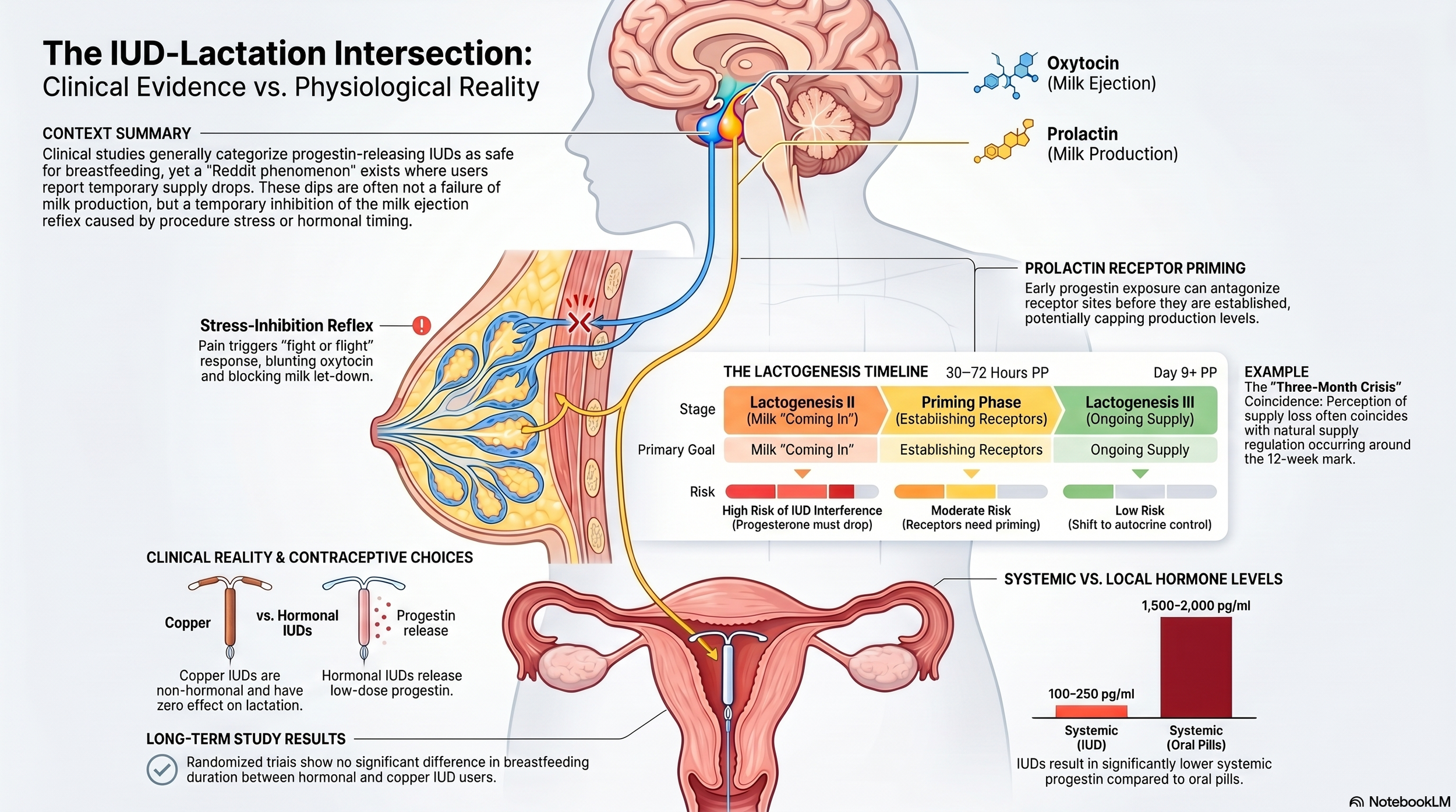
The insertion itself is more than just a minor procedure; it is a significant physical stressor. Clinical documentation notes that insertion can be associated with pain, bleeding, and neurovascular episodes like bradycardia. These events trigger a reflexogenic response. From a neuroendocrinological perspective, acute pain and stress can temporarily inhibit the release of oxytocin, the hormone responsible for the milk let-down reflex. This inhibition effectively "stalls" the delivery of milk, even if the supply is technically present, explaining why many mothers notice a dip within hours of leaving the clinic.
Beyond the immediate procedure, we must consider the pharmacology of the device. Mirena contains a 52 mg reservoir of Levonorgestrel, a progestin. It is designed to release an initial rate of approximately 20 μg/day directly into the uterus. While marketed as a "local effect," the manufacturer’s own data reveals that a stable plasma level of Levonorgestrel (150–200 pg/mL) is achieved within weeks. The systemic reach is documented in the prescription notes:
"Small amounts of progestins pass into the breast milk of nursing mothers, resulting in detectable steroid levels in infant plasma... isolated cases of decreased milk production have been reported."
Crucially, as a mother myself, I must highlight a safety insight often glossed over in the exam room: the Mirena label explicitly warns that the risk of uterine perforation (where the device pierces the uterine wall) is significantly increased in lactating women. This physical risk is a specific consequence of the postpartum, lactating state that every mother deserves to know before consenting to the procedure.
Lastly, this study reports that “LNG-IUD is also associated with altered systemic physiological responses to stress….women using LNG-IUD have substantially potentiated free cortisol and heart rate responses during moderate psychosocial stress compared to oral estrogen-progestin contraception or natural cycling”. This suggests that the LNG-IUD does not just act locally in the uterus, but can affect how the body handles psychological stress, potentially increasing sympathetic nervous system reactivity. This claim is consistent with another study “suggesting a 34 percent higher risk of depression in women using the LNG-IUD”.
The Statistical Probability vs. The Anecdotal Reality
Large-scale clinical trials, specifically those in Finland and Sweden involving over 1,100 women, found no general adverse effects on breastfeeding performance or infant growth. For the vast majority of women, Mirena and breastfeeding coexist without incident.
However, the "Reddit reality" reveals a persistent subset of "isolated cases" where supply drops by 50% or more within 24 to 48 hours. This discrepancy is likely rooted in the clinical pharmacology of metabolic clearance. The rate at which an individual body processes and clears Levonorgestrel can vary several-fold. For a mother with a slower metabolic clearance rate, a "low-dose" device may result in a systemic hormonal concentration that her body misinterprets as a signal to downregulate milk production.
For some, the supply only returns once the hormonal source is removed. As one mother documented:
"I had a Mirena placed and within 24 hours supply tanked. It took twice as long to pump half as much. I waited 5 days, supply didn't return, so I had it removed. 24 hours later supply was right back up to normal."
The 3-Month "Regulation" Crisis
A major confounding factor in these reports is the "three-month breastfeeding crisis," which often aligns with the timing of IUD insertion (typically 6–12 weeks postpartum).
Early milk production is endocrine-driven, fueled by the massive hormonal shifts of birth. By roughly 12 weeks, the body transitions to an autocrine system. This is a demand-based regulation where milk production is managed locally within the breast. During this shift, breasts often lose their constant "engorged" feeling and become "soft" or even "sagging."
It is vital for mothers to distinguish between natural regulation and a hormonal dip. Soft breasts do not equal a lack of milk; they indicate a regulated supply. The true red flag is not the "feel" of the breast, but a sudden, sustained drop in pumping volume such as consistently getting only half of your usual output or a baby who is suddenly unsatisfied after every feed.
Meanwhile, it is worth keeping an eye on other confounding factors like stress or lack of sleep, poor nutrition, herbal supplements (high quantities of pperpmint, sage, or parsley), deficiencies (iron, B12, Vit D, Iodine/minerals, electrolytes), and “period dip” (low calcium/magnesium) that can tank the supply.
The Consequence of the "Tank": When the Risk Becomes Reality
When the supply drop is real, the emotional and physical toll is immense. Mothers often find themselves in a cycle of "all-day nursing" as the infant desperately signals for more milk. To combat this, many resort to power pumping, a rigorous protocol of pumping for 10 minutes, resting for 10, and repeating. While exhausting, this mimics "cluster feeding" to stimulate a surge in prolactin, the hormone responsible for milk synthesis.
If these efforts fail, the emotional toll of needing to supplement with formula against the original birth plan can feel like a profound loss. In these cases, removal of the device is a valid medical choice to preserve the breastfeeding relationship. Many who switch to a non-hormonal option, like the copper IUD, see their supply return to 70–100% of previous levels within days.
The Empowered Choice
The relationship between Mirena and breastfeeding is a complex tapestry of "usually" and "rarely." While clinical studies suggest the device is safe for most, the mothers whose individual metabolic rates or timing create a genuine breastfeeding crisis shouldn’t be dismissed either.
Until women’s health is well-studied and -understood by scientists and clinicians, Mothers are required to be their own primary investigator. Monitor your data, recognize the shift to autocrine production, and understand that while the hormone dose is small, your body’s reaction to it is scientifically valid. If your supply drops suddenly and does not rebound with hydration and prolactin-stimulating power pumping, you have every right to work with your provider to find a contraceptive that honors both your health and your nursing journey.