

The 70kg Man Problem: How Drug Dosing Fails Women
By Whuman Health
As a scientist I know, at a molecular level, how ibuprofen works and yet for as long as I can remember, it has never worn off on the schedule the label promises. This became more evident during my pregnancies when the epidural lingered well past the 24 hours my care team expected.
It wasn't until I started searching the literature that I found the real explanation. The effects I had been experiencing my whole life had a clear, documented biological basis. It was my sex.
I went looking for a tool that could tell me what the right dose actually was for a body like mine and found nothing. No calculator, no clinical resource, no simple guide. Just a wall of research papers that hadn't made it anywhere near the pill bottle.
And here is the why and what behind it:
In 2013, the FDA made a startling admission: women had been overdosed on the sleeping pill Ambien for twenty years.
The reason? Women metabolize the drug nearly 45% more slowly than men. It was building up in their systems overnight and impairing their driving the next morning. The FDA's fix was simple: cut the dose in half for women. What took two decades to correct was a fundamental assumption that had gone unquestioned since the drug was approved: that a woman's body works the same way as a man's.
It doesn't. And Ambien is far from the only drug where this matters.
Why Women Were Left Out of Drug Research
Until the 1990s, women of childbearing age were routinely excluded from clinical drug trials. The intention was protective, regulators were wary after the thalidomide disaster of the 1950s caused severe birth defects in babies born to mothers who took the drug during pregnancy. But the unintended consequence was that for decades, drug doses were calculated, tested, and approved based almost entirely on male bodies.
The standard research subject was a 70-kilogram man, a figure so entrenched in pharmacology that it has a name: the Reference Man. Drug doses were calculated based on how that body absorbed, distributed, metabolized, and excreted a compound. Women were treated, in effect, as smaller versions of him.
Here's the critical problem with that assumption: the dose printed on a drug label is not simply scaled from a pharmacokinetic profile and divided by weight. While pharmacokinetic properties are sometimes adjusted for weight, actual dosing recommendations rarely are — meaning a woman who weighs less and processes drugs differently doesn't just get a proportionally smaller dose. She gets the same dose as a man, full stop. And sex differences in drug exposure in women are not explained by body weight alone — the differences in liver enzymes, body fat distribution, and kidney function persist even after accounting for size.
Regulations changed in 1993, requiring women to be included in federally funded research. But the legacy of that exclusion runs deep. A 2020 study found that of 86 commonly prescribed drugs with known differences in how men and women process them, the overwhelming majority had no female-specific dosing guidance — despite clear evidence that women were being exposed to higher drug levels and experiencing more side effects.
Woman’s Body Processes Drugs Differently

The differences aren't subtle. They're built into basic biology.
Women absorb drugs differently. Food and medication move through the stomach more slowly in women, which affects how much of a drug gets absorbed and how quickly it peaks in the bloodstream.
Women experience significantly slower gastric emptying and intestinal transit times—averaging 91.7 hours compared to just 44.8 hours in men. This delay is largely driven by progesterone, which acts as a natural muscle relaxant for the GI tract.
Women distribute drugs differently. Women have a higher proportion of body fat relative to muscle. Drugs that dissolve in fat like many sleep aids, anxiety medications, and antidepressants spread more widely through fatty tissue, stay in the body longer, and produce stronger effects at the same dose.
For the patient, this doesn't just mean the drug "lasts longer"—it translates to higher rates of morning-after grogginess, impaired motor coordination, and a higher risk of accidental injury.
Women metabolize drugs differently. The liver enzymes that break down most medications work at different speeds in women than in men. Some drugs are cleared faster; many are cleared slower — meaning they accumulate to higher levels before the body can eliminate them.
CYP3A4, which metabolizes roughly 50% of all prescribed drugs, is significantly more active in females. Conversely, CYP1A2 (responsible for caffeine and olanzapine) is more active in males.
Women excrete drugs differently. The kidneys filter blood more slowly in women on average, so drugs that are cleared through urine linger longer in the system.
The result: women are nearly twice as likely to experience adverse drug reactions as men.
Your Menstrual Cycle Matters Too
Here's something almost no prescribing guidelines account for: the hormones that fluctuate across your menstrual cycle don't just regulate reproduction — they also affect how your liver and kidneys process medication.
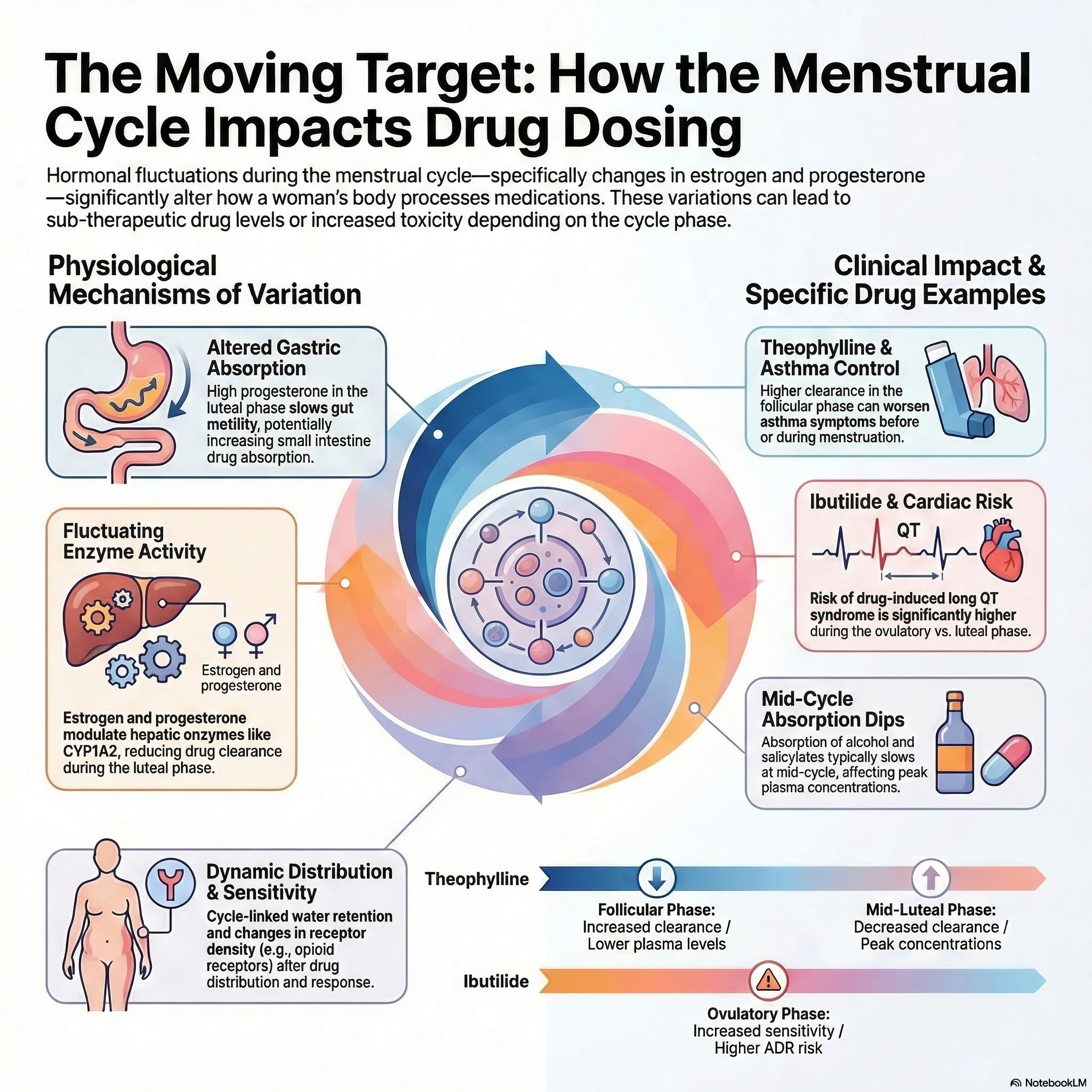
During the first half of your cycle (the follicular phase), rising estrogen slows certain liver enzymes, meaning drugs like omeprazole (a common heartburn medication) and some antidepressants can reach higher concentrations in your blood than they would mid-cycle.
During the second half (the luteal phase), progesterone takes over, changing gut motility, protein binding, and metabolic rates in ways that shift drug levels again. For women with epilepsy, this fluctuation can be the difference between seizure control and breakthrough episodes — carbamazepine levels have been shown to vary by as much as 27% across the cycle.
Even SSRI antidepressants, taken by millions of women daily, may work less effectively in the premenstrual phase — which is why some women with severe PMS are now prescribed cycle-based dosing rather than a fixed daily dose.
For a woman on the pill, a "standard" dose of these medications can effectively become a double-dose.
Guess what, none of this is reflected in the instructions on your pill bottle.
The Scale of the Problem
The numbers are hard to ignore:
8 out of 10 drugs withdrawn from the US market between 1997 and 2000 posed greater health risks to women than men.
31% of new drug applications reviewed by the FDA between 1994 and 2000 showed pharmacokinetic differences between sexes greater than 20% — yet almost none resulted in different dosing recommendations for women.
Women are 50–75% more likely to experience a serious adverse drug reaction than men, across multiple large international databases.
These aren't historical statistics. Most of those drugs are still being prescribed today, at doses that haven't changed.
Introducing a Tool Built for Your Biology
This is why I built the Sex-Adjusted Drug Dosage Calculator — a free tool that translates published pharmacokinetic research into personalized dose estimates for women.
It covers medications with well-documented sex-based differences, including common pain relievers, sleep aids, heart medications, antidepressants, and more. You can use it in two ways:
Basic mode gives you a quick adjusted dose estimate based on your sex, age, BMI, and kidney function — the four factors with the strongest evidence for sex-based dosing differences.
Advanced mode goes further, accounting for your menstrual cycle phase, whether you're on the pill or postmenopausal, and checking for potential contraindications with your existing conditions or medications.
Every adjustment is grounded in peer-reviewed research, with the scientific rationale available if you want to dig deeper.
[←Try the Calculator]
One Important Note
This calculator is an educational tool, not a prescription. Its purpose is to help you understand how your biology may interact with a standard dose — and to give you the information you need to have a better conversation with your doctor or pharmacist.
If the calculator suggests your dose may need adjusting, bring it up at your next appointment. Ask questions. The research exists. It just hasn't made it into the guidelines yet — but that's exactly the kind of gap that informed patients can help close.
The Bottom Line
For decades, the standard drug dose was calculated on a body that wasn't yours. The science now clearly shows that sex, hormonal status, and even the phase of your menstrual cycle can meaningfully change how a medication behaves in your body. Yet most prescribing guidelines still treat women and men identically.
You deserve dosing that reflects your biology. This calculator is a step toward that — and a reminder that asking questions about your medication is not just reasonable. It's necessary.
This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making changes to your medication.
Sources: Zucker & Beery, Biology of Sex Differences (2020) · Soldin & Mattison, Clinical Pharmacokinetics (2009) · FDA Drug Safety Communication on Zolpidem (2013) · Rathore et al., NEJM (2002) · Franconi et al., Expert Opinion on Drug Metabolism & Toxicology (2025)