

Considering GLP-1s (Ozempic / Mounjaro) for Fertility: What to Know Before You Start
By Whuman Health
Heard about “Ozempic babies” and wondering whether GLP-1 medications could help you get pregnant faster? Fertility journeys are often long, exhausting, and isolating, and the pull toward shortcuts is understandable. But GLP-1s don’t work the same way for everyone. Understanding how they affect fertility, who they help, and when they can backfire is essential to avoid delays and frustration on your path to pregnancy.
Who May Benefit From GLP-1s for Fertility
Because GLP-1 medications are primarily used for weight loss and improving insulin sensitivity, the group of women most studied so far includes those with PCOS and those who are overweight or obese, typically with a BMI ≥ 27 kg/m². This represents nearly 40% of women of reproductive age.
But fertility challenges are not limited to women with higher BMIs.
GLP-1s and Fertility in “Lean” Women
“Lean” women (BMI < 27 kg/m²) also experience infertility—often driven by stress, aging, inadequate nutrition (from chronic dieting or over-exercise), or sometimes labeled as “unexplained.” Regardless of body size, nearly all infertility conditions converge on a critical brain region: the hypothalamus.
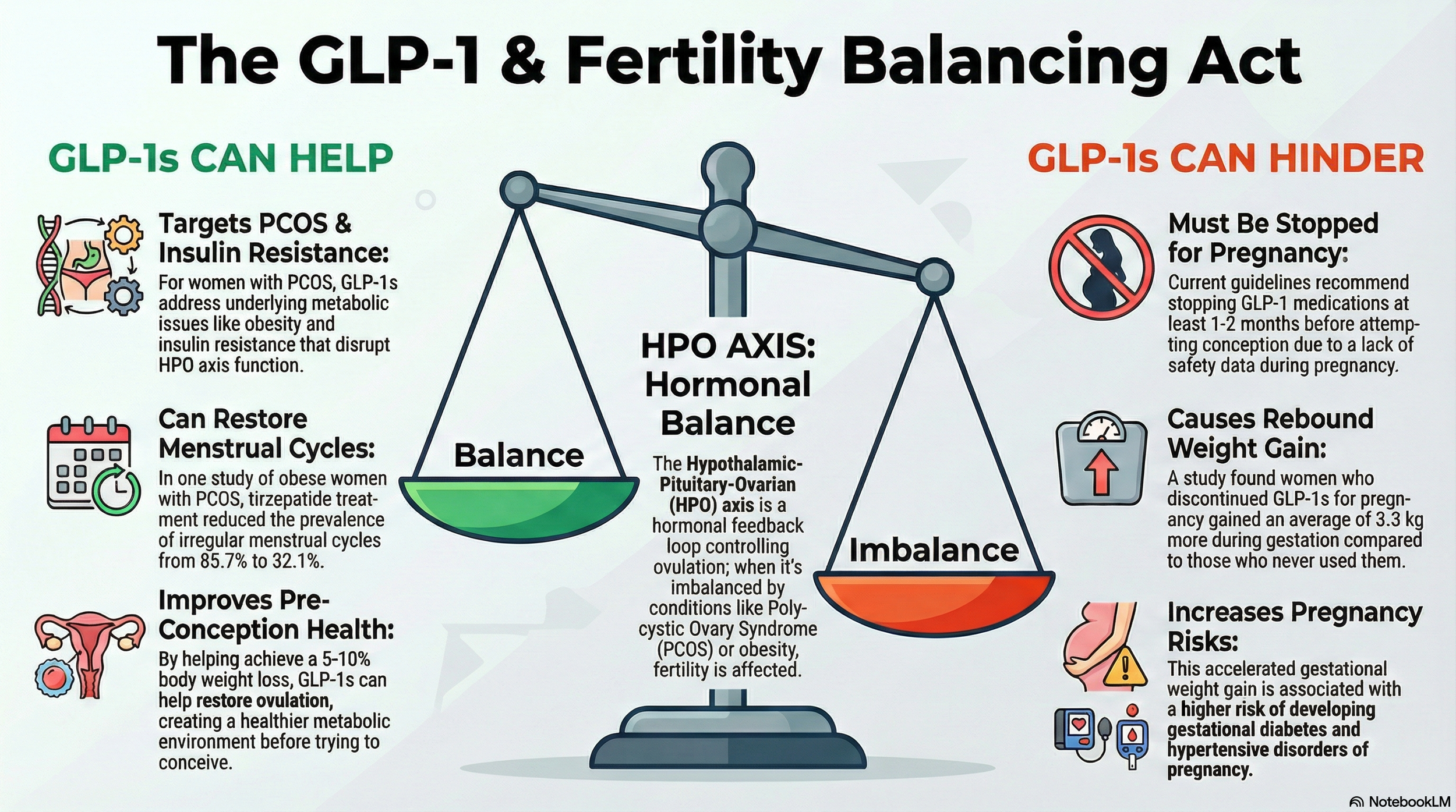
This is where the Hypothalamic–Pituitary–Ovarian (HPO) axis comes in. Almost every major cause of female infertility intersects this axis—either by disrupting GnRH, LH, or FSH signaling, or by altering ovarian hormone feedback. This is where subtlety, balance, and homeostasis matter.
When GLP-1 Medications May or May Not Help Female Infertility
Below is a summary of common infertility causes and when GLP-1s may be helpful.
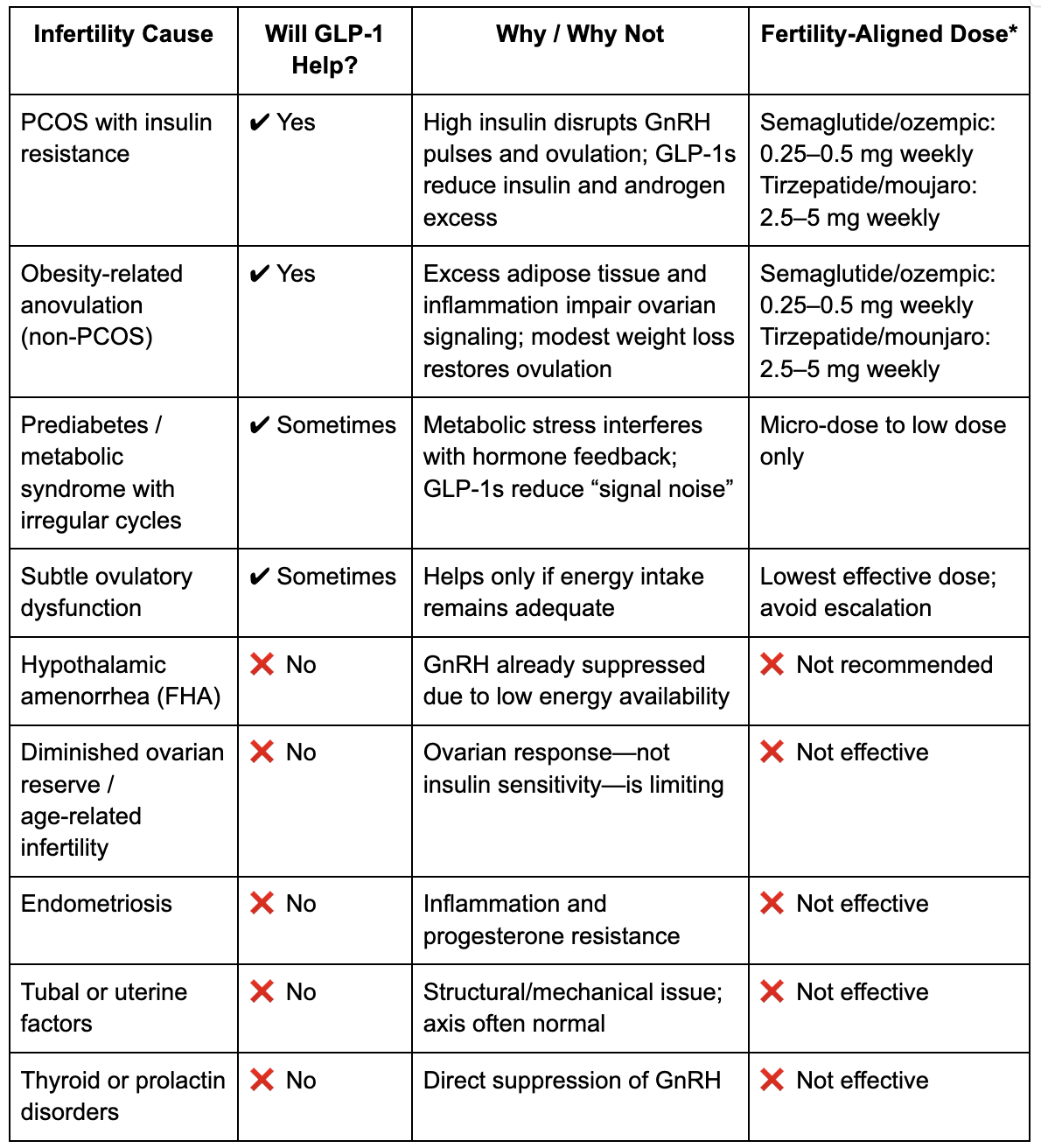
*All GLP-1 medications must be discontinued at least two months before trying to conceive and should never be used during pregnancy. This recommendation reflects the drugs’ long half-lives and animal data showing fetal growth risks at human-equivalent doses. Although tirzepatide/Mounjaro is a different molecule, most reproductive endocrinologists apply the same two-month washout window to protect early organ development.
When to Recalibrate or Stop GLP1?
Knowing when to stop or recalibrate GLP-1s is as important as knowing when to start. These medications support fertility only while they improve metabolic signaling without suppressing ovulation. Once they compete with energy availability, progesterone production, or brain–ovary communication, recalibration—or stopping—is necessary.
Use this checklist to assess whether a GLP-1 is still supporting fertility—or beginning to interfere with it.
🟢 You may be ready to stop or down-titrate if:
Cycles are regular (26–35 days)
Ovulation is consistent
Luteal phase is stable (10–14 days)
Weight loss is ~5–10%
Metabolic markers have improved
At this point, the primary fertility benefit of GLP-1s has likely been achieved.
⚠️ You should strongly consider stopping or lowering the dose if:
Periods become irregular or stop
Cycles lengthen unpredictably
Luteal phase shortens (<10 days)
Progesterone trends downward
Eating enough feels difficult
Fatigue, cold intolerance, or hair shedding appears
Weight loss continues unintentionally
These are signs of hypothalamic suppression, meaning fertility signaling may be turning off.
Pregnancy After GLP-1s: What Happens If Exposure Occurs
What if you discover you’re pregnant while still taking a GLP-1?
A multicenter prospective study (Dao et al., 2024) followed 168 pregnancies with first-trimester GLP-1 exposure. Overall rates of major birth defects (2.6%) were similar to diabetic (2.3%) and obese (3.9%) control groups. However, the sample size was small, and confidence intervals were wide—underscoring the need for continued caution.
Notably, elective terminations were higher (18%) in the GLP-1 group, driven largely by patient anxiety rather than medical necessity. Infants were also more likely to be classified as large for gestational age, reinforcing that the mother’s underlying metabolic health continues to shape the fetal environment long after the drug is discontinued.
Navigating the Transition Off GLP-1s
Stopping a GLP-1 is rarely as simple as skipping a dose. Many women report that once the medication is stopped, appetite “noise” and insulin resistance return quickly. This transition can be especially challenging because pregnancy itself becomes progressively insulin-resistant as placental hormones rise.
Women frequently describe a difficult adjustment: suddenly needing to eat regularly after months of appetite suppression, while simultaneously managing weight changes and glucose control. Without a plan, this rebound can increase the risk of gestational diabetes later in pregnancy.
For a deeper dive into clinical trial outcomes, check out this review article.
Navigating the Consultation: Your Fertility Roadmap
If you’re considering GLP-1s as part of your fertility journey, working with a multidisciplinary team—an endocrinologist, OB-GYN, and registered dietitian—can be invaluable.
Questions to ask your care team:
Given the two-month washout rule, how will we manage insulin resistance between stopping the medication and conception?
Is my infertility driven by elevated LH or metabolic signaling—and could this medication help address both cycle irregularity and cognitive symptoms?
Should metformin be used during the transition off GLP-1s?
What is our plan for managing insulin resistance as placental hormones increase later in pregnancy?
Conclusion
We are witnessing a paradigm shift. Infertility is no longer viewed solely as a reproductive failure, but increasingly as a metabolic signal. For some women, restoring internal balance through GLP-1s can help unlock ovulation and cycle regularity.
But these medications are powerful tools that demand precision, timing, and respect for the transition into pregnancy. Used thoughtfully, they can support fertility. Used indiscriminately, they can delay it.
At Whuman, we believe fertility is not something to force — it’s something to support by restoring the body’s signaling, not overriding it.